

Intrapartum Skills Lab
We have created a 4-station skills lab for midwifery students and ob-gyn residents that includes 1) AROM and placement of a fetal scalp lead, 2) labor support techniques, 3) manual removal of the placenta and bimanual compression, and 4) cervical dilation and effacement, and station of the vertex, and placement of an intrauterine pressure catheter.
An initial pre-brief is held for about 20 minutes. The 4 stations that learners will rotate through are introduced, learners introduce themselves and are divided into 4 groups with a similar number of residents and midwifery students in each group. The groups rotate through each of the 4 stations approximately every 20 minutes. A faculty member teaches each station, we use 2 midwifery faculty and 2 ob-gyn faculty.
- AROM and placement of a fetal scalp lead: this station uses a model found online for this skill. A can cozy, saran wrap and orange are needed as well as an amnihook and a scalp lead. Shown in this video. An explanation of the technique is provided by the faculty member, each learner has an opportunity to try the technique.
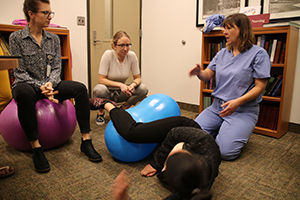
- Labor support techniques: a number of labor support techniques are described and demonstrated by a faculty member including use of a birth ball, peanut ball, rebozo, counter pressure, hip squeeze, effleurage, and other techniques as selected by faculty. Learners practice the techniques with each other.
- Manual removal of the placenta and bimanual compression: a task trainer pelvic/uterine model with a placenta is needed for this activity. We currently use the Paradigm birthing model which comes with a separate postpartum uterus and placenta that is more realistic for manual removal. Faculty member describes and demonstrates. Video can be seen here.
- Cervical dilation and effacement, and station of the vertex, position of the vertex and can include abnormal such as face, brow; and placement of an intrauterine pressure catheter: a birthing model with ability to have cervices at different effacement and dilation, ability to palpate sutures and fontanelles, and ability to palpate spines to determine station. We have used the Prompt and Mama Birthie Models.
A checklist has been developed to make sure learners experience all aspects of these skills stations including communication with the client.
Checklist for labor support skills
- Assess coping, introduce to Coping with Labor Algorithm
- Ask woman what would be helpful or if she would like to try specific tools
- Demonstrate and practice birthing ball to sit on, use near side of bed, on bed
- Demonstrate use of peanut ball for women with epidural, other
- Demonstrate use of rebozo
- Demonstrate hip squeeze, effleurage, counter pressure to lower back
After all learners have completed all 4 stations, everyone comes together for a debriefing session of 30-40 minutes. Learners are asked questions such as their impressions in general, what they learned, what they learned from each other, often discussion arise related to the preparation and scope of practice and education pathways of ob-gyns and midwives. We have assigned a couple of our modules and readings on collaborative practice in advance of the session.
IPE Objective Structured Clinical Experience (or can be Examination)
We have developed a 3 station OSCE for 2nd year residents and midwifery students in their 2nd of 3 semesters of intrapartum/4th of 5 semesters if clinical experiences.
Three stations or clinical cases have been developed where a resident and a midwife student enter a patient room together and interact with a standardized patient (SP) playing a specific developed case. All case details are written by the midwifery and ob-gyn faculty, our simulation lab staff bring it to life with equipment and materials and train the SPs for the cases. Each case lasts 20 minutes. Learners undergo a pre-brief with an icebreaker activity to begin the session, about 20-30 minutes. Then each resident/midwife student pair cycles through each of the 3 cases. After all cases are complete, learners complete a debrief session with sim center staff where they talk about what went well, what was difficult, what they learned about themselves and each other, what can be improved about the learning experience. Faculty contribute to the debrief as well.
The cases were developed to have both ambulatory and labor/birth simulations, to have situations where each of the ob-gyn and midwife might have additional expertise to provide consultation. The three cases are 1) anticipated shoulder dystocia (SD) in which a woman has a fetus with a large EFW, and history of a previous SD; the ob-gyn is asked to attend the birth with the midwife, a SD ensues and newborn resuscitation is also required, 2) a woman at 8 weeks postpartum has returned to work and is concerned about low milk supply, trying to pump at work, and has been a physician patient during her pregnancy. Midwife is asked to attend the visit with her ob-gyn to help with breastfeeding concerns, and 3) a woman has had several hours of lack of progress of cervical dilation in active labor at a freestanding birth center. She is transferred from her birth center midwife to the hospital midwife and the hospital midwife and ob-gyn see her together to asses her situation and work with her to determine next steps.
[These structured clinical experiences were created as part of a funded project prior to the Macy-funded IPE project and continued in the Macy project.]